 阿摩線上測驗
阿摩線上測驗
34.62歲男性,有DM、CKD stage 4病史。下列何者治療其慢性胰臟炎之處置最不適當?
(A)疼痛控制,meperidine
(B)血糖控制,insulin glargine
(C)腸胃道吸收不良,pancreatic enzyme
(D)steatorrhea,famotidine
答案:登入後查看
統計: A(1503), B(145), C(199), D(543), E(0) #3133801
統計: A(1503), B(145), C(199), D(543), E(0) #3133801
詳解 (共 10 筆)
TMU b323109053
#6122943
可能會有人想知道為甚麼第四個選項是對的 (這題真的很可愛),因此在這邊我想說說看我的推測:
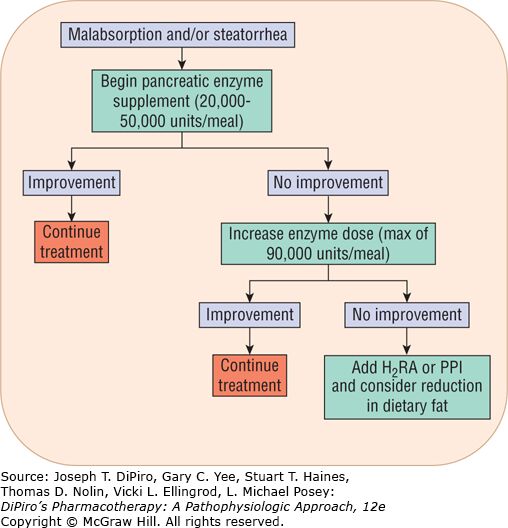
在 DiPiro’s Pharmacotherapy: A Pathophysiologic Approach, 12th Edition 的chapter 57 pancreatitis 之 figure 5,大家可以看到最下面有寫:如果enzyme的劑量已經到達最大,但還是沒有效果,那可以加上H2 bloker or PPI 來試試看。那這可能是因為他們想要利用制酸劑來降低enzyme被胃酸去活化的部分,以保留較多的活性enzyme。
p.s 在胰臟炎想要止痛的話,急性時優先使用opioids類 (morphine, fentanyl, hydromorphone...);慢性的話就會跟一般的疼痛治療一樣使用階梯療法 (acetaminophen / NSAID → 弱鴉片類 + acetaminophen → 強效鴉片類)
pp.s 關於pancreatic enzyme的重點:
- 如果對豬製品過敏的病人就要注意不能使用pancreatic enzyme
- Hyperuricemia, Fibrosing colonopathy (doses greater than 10,000units/kg/day) → 常見的pancreatic enzyme副作用
- 懷孕的人不能吃pancreatic enzyme!
74
0
Namaste
#6285953
Meperidine用於「急性」疼痛控制
較不適合用在PCA。因為其半衰期短、會產生毒性代謝物normeperidine,用在PCA中會提高發生藥品中樞神經副作用(例如:癲癇)的風險,也不適用於腎功能不佳的病人
fentanyl:腎衰竭病人之PCA首選
8
0
美美黑
#6139618
慢性胰臟炎主要有兩大併發症,即脂肪痢(大便有惡臭味)及糖尿病,胰臟是負責分泌:胰澱粉酵素(amylase)、脂解酶(lipase)、蛋白酶(Protease)
優妙化膠溶微粒膠囊(PANCRELIPASE):Pancrelipase 280mg ( Lipase 20000 USP Units、Protease 75 000 USP Units、Amylase 66400 USP Units )
衛署適應症:纖維性囊腫、慢性胰臟炎、胰臟切除、胃腸鏡道手術及
因腫瘤引發胰管式膽管阻塞等疾病所導致的胰液分泌不全。
7
0
嬤的髮刻
#6013725
即便在癌症疼痛控制上有類似的考量
uptodate:
Meperidine — Meperidine also is not preferred for use in the cancer pain population. It is metabolized into a compound (normeperidine) that is relatively toxic, and associated with tremulousness, delirium, and seizures. The metabolite has a longer half-life than the parent compound, and its concentration in blood rises for several days with repeated administration. Some patients will therefore develop normeperidine toxicity with repeated dosing over days. The metabolite is renally excreted, and its concentration increases (with greater risk of toxicity) in the setting of renal insufficiency. It is safer to select an alternative mu agonist for the management of chronic pain.
5
3